
Tick-borne Disease in Maine (Part Two): Two Standards of Care

Author: Paula Jackson Jones
Orig Published: 09/21/2017
With
an increase in Lyme and tick-borne cases, patients are reporting a variance in
how they are or are not being treated. Why?
The simple answer is that there are TWO STANDARDS OF CARE, however, the
reality is that it’s far more complicated than that. I’ll do my best to explain
this is layman’s terms and not get too overly complicated.
The
History of Lyme Disease
In
the early 1970’s, a group of children in Lyme, CT were suffering from puzzling
and debilitating health issues. Initially diagnosed as Juvenile Rheumatoid
Arthritis but when visits to doctors and hospital stays became more frequent, two
mothers from this group became persistent in finding answers and began
conducting their own research and contacting scientists. By the mid-70’s,
researchers had collected enough data including signs and symptoms and called
it Lyme, but they didn’t know what caused it.
In 1982, a scientist by the name of Willy Burgdorfer, who was studying
Rocky Mountain Spotted Fever at the time, began studying Lyme and soon made the
connection between the deer tick and Lyme. He discovered that a bacterium
called a spirochete, carried by ticks, was causing Lyme and in 1982 the medical
community honored his discovery by naming the spirochete Borrelia burgdorferi (Bb).
Now
I’m going to pull out the highpoints:
Initial
criteria for diagnosing and treating were set by the Infectious Disease Society
of America (IDSA) and then reviewed again in 2006 without change. During this
time, another group emerged presenting an equal amount of scientific evidence
that spoke to the concerns of delayed diagnosis and improper treatment as
contributing to the growing population of patients who remained sick, some with
chronically debilitating symptoms. This
group was called International Lyme and Associated Diseases Society (ILADS) and
consisted of highly educated physicians and researchers with first-hand
experience with Lyme and tick-borne disease. Over time and with further
research, evidence was produced that patients who were not properly diagnosed
and treated early, required a different kind treatment. Evidence that spoke to
the myriad of symptoms between adults and children, acute cases versus chronic
and late stage and the complications co-infections of another tick-borne
disease could cause. It became very
apparent to this group that applying a one-size-fits-all approach to treating
was not the best course of action and so they began to write their own set of evidence-based
guidelines and treatment protocols and training medical doctors accordingly.
Thus,
began the controversy with Lyme Disease.
The IDSA does not and has not since their conception, recognized the
validity of ILADS, their medical providers and any of the evidence that they
have provided. They claim that their
science and evidence is truth and upholding and any other evidence presented is
dismissed. Back in 2006, when the
initial IDSA guidelines went under review, a huge medical storm was brewing. It
was during this time that fingers were pointing and accusations were flying of
misappropriate conduct. And even given the amount of new evidence being
provided by members of ILADS and other researchers, the IDSA guidelines were
deemed adequate and therefore, no need for change.

In
2010, Congressman Chris Smith (NJ), Chairman of the House congressional panel
that oversees international global health issues introduced a Congressional
Record report that exposed research gaps in Lyme Disease. Then in 2012, a
congressional hearing was held by Congressman Smith, who sponsored federal
legislation to expand federal efforts on Lyme and other tick-borne disease
through the establishment of a Tick-borne Disease Advisory Committee.
Congressman Smith stated the following:
“As I have met
scores of patients suffering the devastating effects of Chronic Lyme—who only
got well after aggressive treatment by a Lyme-literate physician—I have been
dismayed and angered by the unwillingness of some to take a fresh,
comprehensive look at this insidious disease. It will be necessary for the
physicians, scientists, government leaders, and media to be discerning – to
evaluate the evidence to see if it is based on the best science and to
scrutinize the studies and the critiques of those studies to determine whether
they are of high quality. We need scientists to speak out in an
unfettered way. We need government agencies to show leadership and to forcefully
say what we know and what we don’t know based on the best available evidence.”
The
controversy over the two standards of care has gotten so bad that doctors have
reported other doctors for what they feel is medical misconduct. I’ve spoken to
providers who call ILADS doctors “quacks” saying that they are self-proclaimed
“experts” calling themselves Lyme literate, practicing without science and
treating with snake oil.
Well,
the National Guidelines Clearinghouse thinks otherwise.
The National Guidelines Clearinghouse (NGC) is an initiative
of the Agency for Healthcare Research and Quality (AHRQ), under the umbrella of
the U.S. Department of Health and Human
Services. The NGC recently adopted the Institute of Medicine (IOM) standards
for developing trustworthy guidelines, which define the highest level of
excellence that a guideline can achieve. Guidelines posted on the NGC website
must now satisfy these standards. Thus, the inclusion of ILADS’s peer reviewed
guidelines on the NGC website demonstrates that they meet the level of
excellence called for by the IOM."

In the fall of
2015, ILADS guidelines were accepted into the NGC database and in February of
2016, the IDSA guidelines were removed after many requests for updates and to
this day, they have not been re-added.
Fast
forward to today. You have a patient who
remains sick, who didn’t respond to the initial course of treatment. Maybe they didn’t present with the classic
qualifying symptoms or lab results were initially negative. Maine LD422 passed
into public law in 2015 and allows for a provider to treat “alternatively”. The
Maine CDC has both the IDSA and the NGC links on their website. Even the
outdated IDSA guideline footnote states “adherence is not mandatory nor is it
to supersede a physician knowledge and individual patient situation”

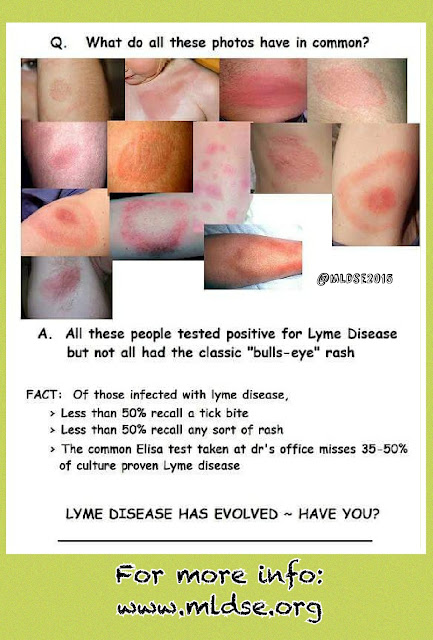
Lyme and
tick-borne disease has evolved and is on the rise here in Maine. The best
defense, first and foremost, is prevention but if exposed to a tick-borne
disease, you want a medical provider using up-to-date diagnostic tools and
treatment options.
~ Paula


Comments
Post a Comment